NIPPLE-AREOLA COMPLEX RECONSTRUCTION
- Homepage
- RECONSTRUCTIVE SURGERY
- BREAST
- NIPPLE-AREOLA COMPLEX RECONSTRUCTION
Nipple-Areola Complex Reconstruction
Occasionally your own nipple can be preserved safely, but a mastectomy usually involves removing the whole breast including the nipple and areola. It’s possible to have the nipple reconstructed and this may be done at the same time as the breast surgery. However, it’s more commonly done a few months after the reconstruction to give the new breast time to settle into its permanent position and to make sure you’re happy with the symmetry of your breasts. The Nipple Reconstruction can be done under a local anaesthetic if carried out after the Breast Reconstruction.
A reconstructed nipple can improve the appearance of your new breast, but it won’t feel the same as a natural nipple. It has none of the nerves that allow it to become erect or flatten in response to touch or temperature, and it has no sensation.
- The procedure
There are several ways of reconstructing a nipple, so you may want to discuss different options with Dr. med. Strouthou.
We recommend the following options:
Skate Flap
The Skate Flap Nipple Reconstruction provides good nipple projection, diameter and definition. It uses most of the skin removed to place the areola graft. The wings of the skate flap blood supply come from a well-vascularised subcutaneous pedicle. So, a circle that is equal in diameter to the contralateral areola is down at the NAC future site. The upper third of this circle is delineated as a separate deepithelialisation, the skin is discharged. The lower two thirds will be elevated as lateral and medial wings based in the centre, as an attached vascularised pedicle within the centre of the circle The proper placement of the future nipple is determined and a 50% longer nipple projection is estimated, assuming that it will shrink to perfect symmetry. The wings of the skate flap are deepithelised to the proposed width of the skate flap, and then a cut through the dermis into the subcutaneous is made. This tissue is lifted up, and the wings of the flap are brought around. The areolar graft can be taken from the excess tissue on the lateral portion of the mastectomy or from upper lid or inner thighs. A silicone sheet is applied to stabilise the graft. Normally, tattooing is not required.
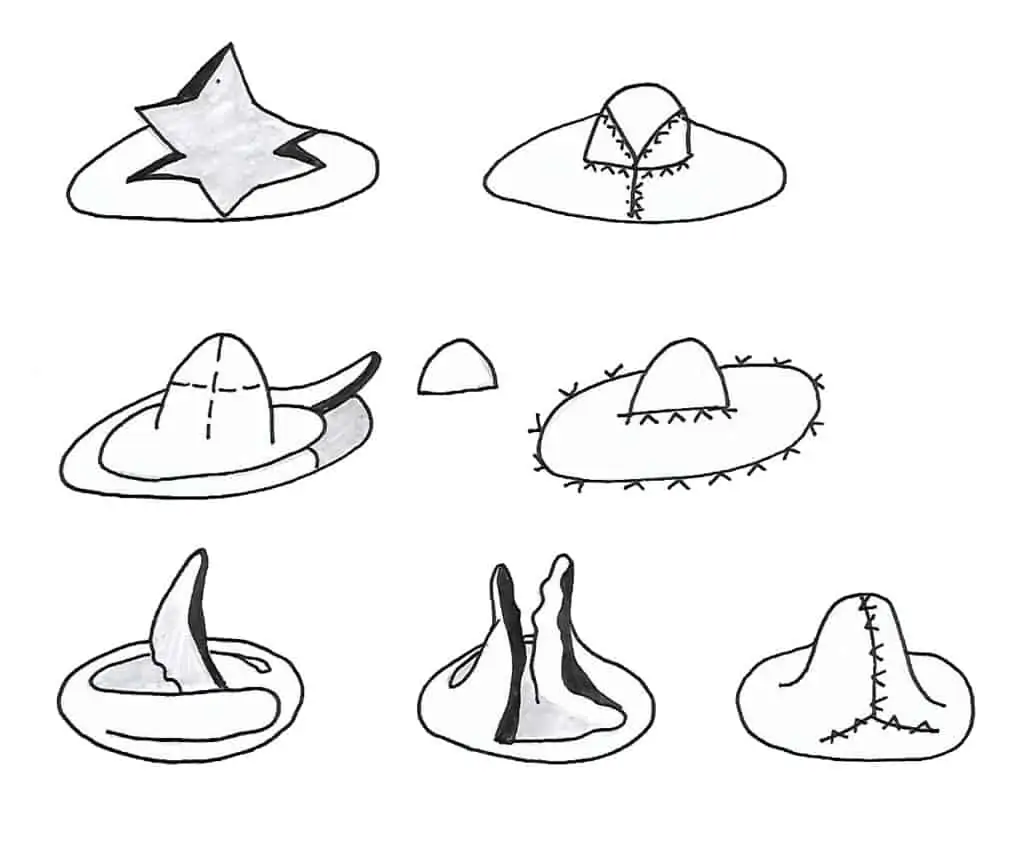
Star Flap
Star Flap is a derivative of the Skate Flap. The tapered arms wrap around a central composite flap to create the nipple papule. The star flap has the advantage of primary closure over the star flap, which usually requires skin graft. The disadvantage is less projection and the three donor site scars. Tattooing is always required for the areola reconstruction.
Tattooing
Tattooing can be associated with other techniques to improve the outcome, providing the right colour and shape to the reconstructed NAC. Some patients prefer this method alone, since they want the quickest, painfulness NAC reconstruction technique. Although colour match and shape can be good, it lacks in texture and projection. Nevertheless, nowadays, with 3D techniques, using principles of light and shadow to create depth on a two-dimensional surface, some tattoo artists can reproduce incredibly realistic nipple-areolar complexes. Pigment fading was the most common long-term complaint, voiced by up to 60%. After a few required touch-ups, the majority were satisfied with their outcome. Tattoo colours may be selected a bit darker to compensate for the predictable changes that will occur. The right technique is also very important. Pigment placed superficially will result in its extrusion and sloughing, and, if placed too deep, it will lead to macrophage ink phagocytosis, both resulting in early pigment fading. Tattooing equipment can be regulated to ensure the right needle depth in the dermis.